Empty space, drag to resize
After wrapping up a dry needling course, one theme kept coming back: risk-awareness in needling.
During the course, two topics came up:
- Navigating the risk of pneumothorax and what happens if it occurs
- How worried should I be about hitting the vertebral artery
These are the kinds of things clinicians quietly worry about. It is something we have been taught to worry about. So this week, I wanted to dig deeper into these concerns—not to scare anyone, but to help all of us needle above the line: confident, safe, intentional, and grounded in reality.
Going through OCS and RCPM
Reviewing Lats, and the Cuff

During the course, a few points of discussion came up where we didn’t leave with as much clarity as we’d hoped. So afterward, I dug back into the research and anatomy texts to get a more accurate picture of what’s actually going on.
In the course follow-up email, Matt Boudreau, PT, and I highlighted two major risk-check items worth revisiting:
1. The risk of pneumothorax when needling the thorax, upper back, or shoulder region—a rare complication, but the one most clinicians worry about, and for good reason. The incidence is well documented in the literature; what felt less clear was the typical management and prognosis for these small, iatrogenic punctures.
2. The concern about hitting the vertebral artery when needling the suboccipital muscles—specifically, how real that risk is anatomically, and what would actually happen if the artery were nicked.

Pneumothorax remains the most clinically meaningful risk in dry needling — but its actual likelihood is low when technique is sound.
The highest-risk zones include:
- Upper trapezius, especially in thin individuals
- Levator scapulae at the superior angle of the scapula
- Rhomboids
- Paraspinals above T7
Most iatrogenic pneumothoraces occur due to:
- Overly vertical needle angles
- Using a needle length that is too long for the patient’s body habitus
- Incomplete understanding of the anatomy and depth
- Clinician fatigue or lapses in attention
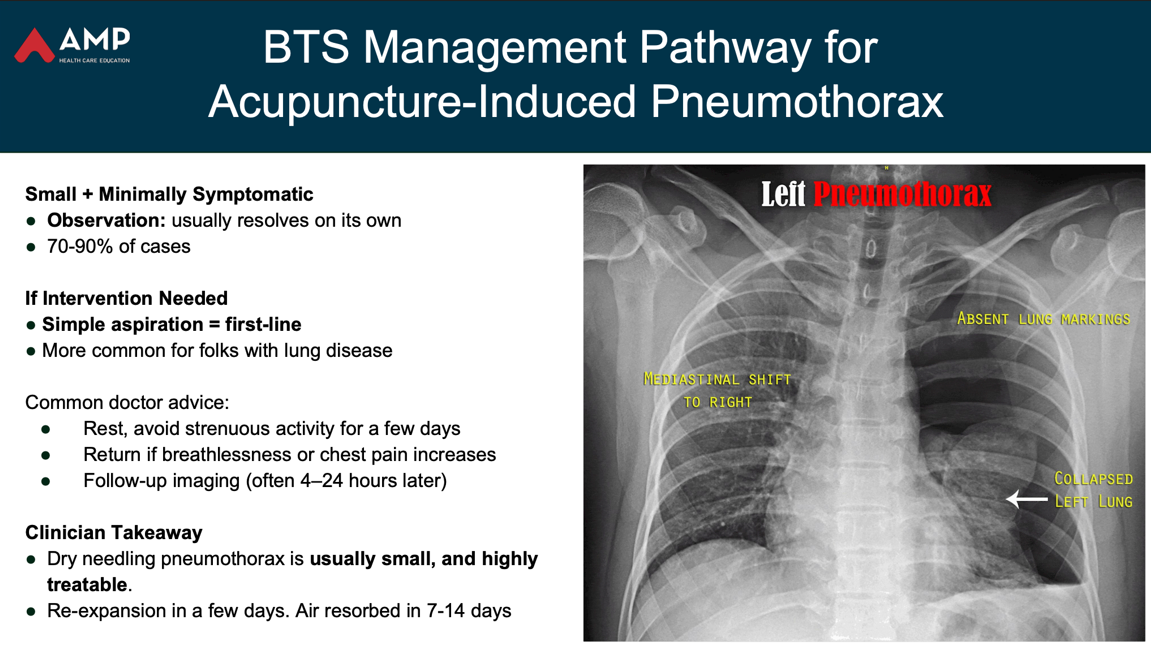
Recovery data is reassuring:
- 70–90% of iatrogenic pneumothoraces resolve with observation alone
- A small proportion require needle aspiration
- Only a few cases progress to needing a chest tube
Key safety points:
Know your backdrop. Know your anatomy. Use the right needle length. Angle appropriately.
- Can a needle reach the vertebral artery?
I revisited this question again recently.
Short answer: No.
With correct dry needling technique, it is anatomically almost impossible for a filiform needle to reach the vertebral artery.
Here’s why — with more detail than I usually like to go into:
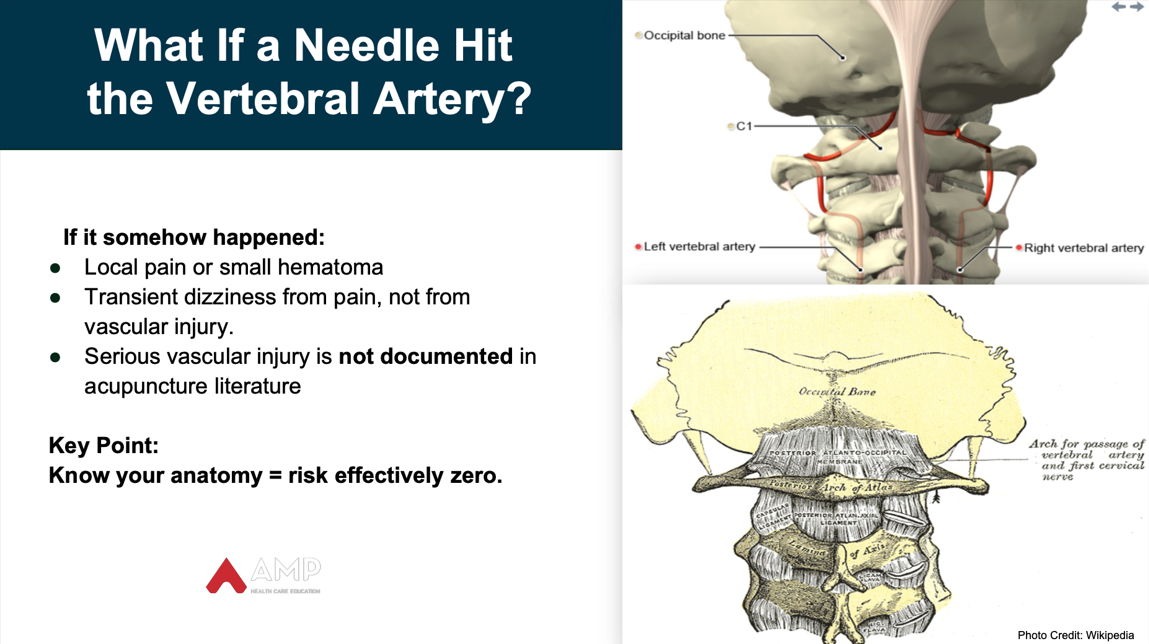
• At C2:
The vertebral artery sits inside the transverse foramen, a rigid bony tunnel that fully encloses and protects it.
→ A needle cannot enter or pass through this osseous canal.
• As it ascends to C1:
The artery exits the foramen and immediately drops into the sulcus arteriae vertebralis, a deep bony groove on the superior/posterior arch of C1.
→ This groove acts like a protective trench that a needle cannot access.
• It is then covered by the posterior atlanto-occipital membrane:
A dense, fibrous ligamentous layer forming a roof over the artery and separating it from all superficial tissues.
→ A fine-gauge acupuncture needle cannot reliably pierce this membrane.
• Above that membrane lie several muscular layers:- Semispinalis capitis
- Splenius capitis
- Obliquus capitis superior
- Obliquus capitis inferior
These layers provide ~2.5–4+ cm of tissue above the artery, depending on individual anatomy.
Bottom line:
For a needle to reach the vertebral artery, it would have to traverse multiple muscular layers, penetrate a tough ligamentous membrane, and then enter a protected bony groove — something filiform needles are not physically capable of doing when used with proper technique and angulation.
That said, prudence and respect for depth, direction, and anatomy are always essential.
Important Note:
I could not find any documented cases of iatrogenic vertebral artery injury caused by acupuncture or dry needling in the literature. If you come across any, please let me know.

A Simple Way to Sharpen Your Safety Mindset and Technical Precision
Step 1: Choose a higher-risk anatomical zoneExamples:
- Upper trapezius or levator scapulae (lung risk)
- Rhomboids (lung risk)
- Suboccipital region / RCPM / OCS (where clinicians often worry about vertebral artery proximity)
Step 2: Before each needling session in these zones, take a 15-second “safety pause” and run through three prompts:
1. Surface Anatomy & Layering- What layers will my needle pass through?
- What vital structures lie deep to my target (lung apex, pleura, artery, nerve roots)?
- What anatomical variations might matter for this patient (e.g., thin build, muscular, osteoporosis, hypermobility, hyperinflated lungs)?
2. Depth, Angle & Backdrop- What is my maximum safe depth for this patient?
- Is my needle angled toward my finger or a bony backdrop, or am I drifting into “free air”?
Step 3: Reflect at the end of the weekReview any notes or small observations. Use them to refine your personal “high-risk zone checklist” or your teaching points if you supervise others. These small insights tend to cluster over time — and they dramatically widen your safety margins.

- Update your informed consent: make sure patients understand rare but serious risks (e.g., pneumothorax), particularly when working near thorax or upper back. Use the framework from Ickert et al. 2024 for good consent language.
- Review real-world evidence: a recent case by Mintken et al. 2025 describes a 24-year-old who developed a moderate pneumothorax after rib-bracketing DN — required chest tube and overnight hospitalization, but fully recovered by one month. This case reinforces the need for vigilance in high-risk zones, consideration of safer technique options, and clear, informed consent.
- Explore deeper training: check out the AMP Healthcare blog “Needles, Consent, and the Fine Print” — a thoughtful look at consent, risk framing, and patient communication.
- Consider structured learning: the AMP Healthcare DN-LP course offers structured content on needling practice, risk identification, and best-practice protocols for the lumbo-pelvic region and lower extremity. Coming April 2026.

It’s always wise to err on the side of caution — but it’s equally important to understand why those precautions exist and what the actual likelihood of harm is. When we pair respect for risk with clarity about its true probability, we make better decisions, communicate with more confidence, and needle with the kind of grounded precision patients deserve.
Empty space, drag to resize
Clients trust us not only to help them feel better, but to keep them safe — especially when we’re working near structures like lungs, vessels, and nerves. This week’s deeper dive into risk is a reminder that safety isn’t a separate part of practice; it is practice. It shows up in how we brief people, how intentional we are with our needle angles and backdrops, and how we monitor and follow up.
When we combine curiosity (about anatomy and variation), competence (in technique and decision-making), and humility (to acknowledge what we don’t know), we widen the margin of safety for everyone in the room. That’s what leads to better outcomes — for both patients and clinicians — and that’s how we keep dry needling both effective and trustworthy.
Stay nerdy,