Empty space, drag to resize
Hey folks,
If you’ve spent time with patients living with persistent pain, you’ve likely seen it—an underlying hesitancy that has nothing to do with strength or structure. They move cautiously and slowly. They may hold their breath. They scan for feedback. There is an attentional and gravitational pull towards their symptoms.
This is discomfort and doubt in action.
This week’s newsletter is about that doubt. Where it comes from, why it matters, and how to work with it—not by labeling it, but by understanding it.

Let’s start with
Bunzli et al. (2017). In this paper, they offer a respectful and useful framing for pain-related fear: fear emerges when someone
can’t make sense of their pain.
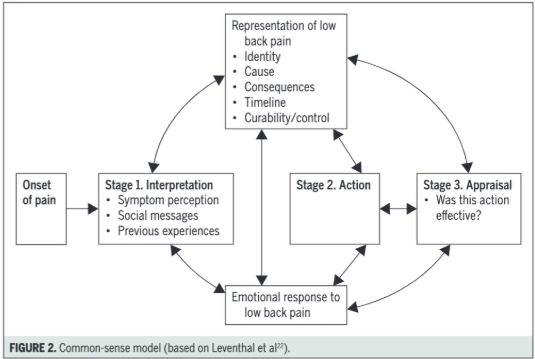
They draw from the Common-Sense Model of Self-Regulation, which describes five domains people instinctively use to interpret symptoms:
- Identity – What is this pain?
- Cause – What started it?
- Consequences – What does it mean for my life?
- Timeline – Will it go away, or is this permanent?
- Control – Can I do something about it?
If one or more of these beliefs is unclear—or doesn’t align with what the person is experiencing—fear tends to fill the gap.
A helpful parallel:
Imagine you’ve just been let go from your job, one that you are exceptional at, without a clear reason. You’re unsure what happened, whether it’s permanent, what it means for your future, or what you’re supposed to do next. You might begin to doubt yourself in areas that used to feel solid. You avoid applying to new and similar jobs, your sleeping starts to tank, and your confidence begins to fray
Pain-related fear is often the same. It can come from confusion and doubting what you thought you once knew so well. When pain shows up without a clear “why,” when it sticks around longer than expected, and when nothing seems to change it, people naturally become protective.
This is normal reaction to an abnormal situation.
So before we offer new movement strategies or reassurance, it’s worth asking:
Does this person have a story about their pain that makes sense to them?

This leads directly into the question: How do fear and belief systems actually influence outcomes? That’s where
Lee et al. (2015) comes in.
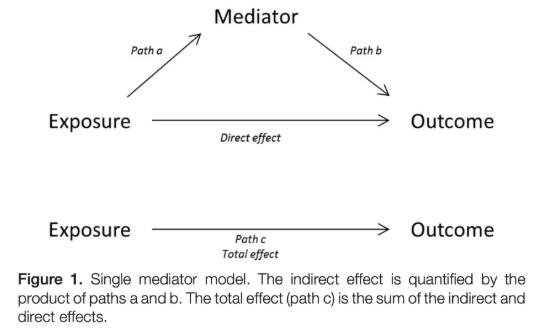
This systematic review looked across 34 studies (n = 2,961) examining the psychological mechanisms that mediate the relationship between pain and disability. In plain terms: what are the levers that matter most?
The standout finding was clear:
- Self Efficacy—the belief that “I can handle this”—was the strongest and most consistent predictor of lower disability. (β = 0.23)
- A beta of 0.23 means that as self-efficacy increases, disability tends to decrease — and the strength of that link (the effect size) is small to moderate.
Also relevant:
- Psychological distress (anxiety, depression) had a smaller but consistent role (β = 0.10)
- Fear of movement or injury had a modest effect (β = 0.08)
- Catastrophizing, often assumed to be central, didn’t show up as an independent factor when other variables were accounted for.
So what does this mean in practice?
It suggests that how capable someone feels is more important than how afraid they are. It’s not fear itself that leads to long-term dysfunction—it’s the belief that they can’t do anything about it.
If pain-related fear is smoke, then loss of agency is the fire.
This should reframe our treatment priorities. Instead of trying to “correct” fearful thoughts, or "explain pain" we focus on building a sense of confidence through experience—through movement, discovery, and proof that life is still accessible.
This sets the stage for what to do next: identify where fear shows up, and start there.

This is where
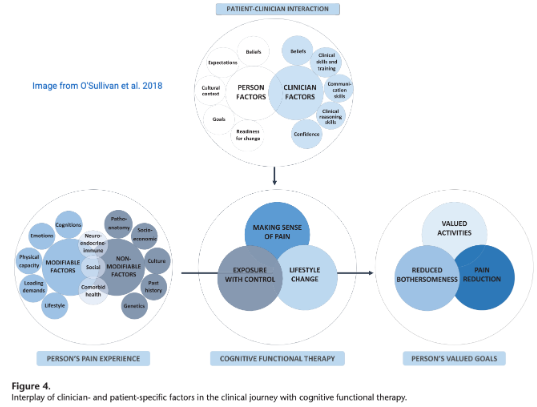
O’Sullivan et al. (2018) comes in. In their practical overview of
Cognitive Functional Therapy (CFT), they show how to spot—and respond to—protective behaviours that might signal deeper fear.
It’s not just what patients say. It’s also how they move:
- Overly controlled or braced movement patterns
- Slow movement
- Avoidance of forward flexion or rotation
- Breath holding during basic tasks
- Flinching or grimacing before a movement or when contact is made
These reactions might be the by-product of the body enacting the person’s current belief system.
Often, those beliefs are shaped by uncertainty, memory and past pain, not present danger. Our job is to notice those patterns and ask:
What story is this person currently living in and how can we help shape a better one?

When working with people experiencing pain, we know recovery isn’t just about tissue — it’s also about beliefs, fears, and the stories we carry. These clinical tools below can help us gently surface and reshape those stories in meaningful ways.
To explore someone’s current narrative, we can ask:
- What do you think is going on with your back?
- What do you think caused it?
- What’s your biggest worry about it?
- How long do you think it will last?
- What helps you feel more in control?
These questions surface more than just fears — they reveal gaps: in understanding, in predictability, in perceived control. And that’s where the intervention starts. Make sure to circle back to these when it comes time for treatment planning.
Rather than telling someone a movement is safe (general reassurance), we invite them to become a scientist in their own lab — testing their beliefs in real time.
Step-by-step:
1. Choose a meaningful task they’ve been avoiding or feel hesitant to do.
2. Elicit a prediction:
“What "What do you think might happen if you do that movement?”
3. Settle the system with a few relaxed breaths.
4. Explore the movement with less guarding or in a novel way (e.g., slower, different posture, attention shift).
5. Reflect after:
- “What was that like?”
- “Was it what you expected?”
This process mirrors the scientific method: form a hypothesis, test it, observe the outcome, and update beliefs. Each time a fear isn’t confirmed, we create an opportunity for unlearning and learning. This is how we create embodied reassurance.
Every movement completed is a
micro-proof: you can.
By helping patients notice and name these wins — and track them across time and multiple contexts — we build confidence. As they gather evidence of capacity, avoidance gives way to more participation, more curiosity and more "experiments."
We’re not just helping people move again — we’re helping them regain predictability and controllability of their situation.
🎥 This video offers a glimpse of how this approach feels in real-life clinical encounters.
Fear doesn’t live in the tissue — it lives in the space between experience and explanation.
When someone can’t make sense of their symptoms, even familiar movements can feel risky — like every step is a gamble.
The solution isn’t to correct them. It’s to help them build a map — one that makes sense of their body, their experience, and their pain.
As clinicians, we shift too — from being the fixer to being a coach and scientist alongside the patient. Together, we form hypotheses, elicit predictions, run small experiments, gather evidence, and update beliefs. This is shared inquiry into safety, agency, and possibility.
And what emerges through this process is more than pain relief. It’s a
re-occupation of self, as
Thompson et al. (2020) describe — where the person makes sense of their pain in a personally meaningful way, reclaims their identity from “patient” to “person,” and begins to flexibly persist through life again.
We help them navigate — not always back to how things were, but toward a place where their body feels familiar, capable, and safe again — even if that means accepting a new version of normal.
Fear with pain isn’t the enemy. It’s a signal — pointing to a gap in coherence, in confidence, in control.
I get really curious when I notice movement hesitancy, grimacing when talking about a specific activity or off-hand comments that hint at avoidance. I listen closely for what hasn’t been clearly articulated yet — the quiet story beneath the surface.
Because when we invite people to test their story, we do more than reduce pain. We help them unlearn what no longer serves — and learn something new about what they’re capable of.
