Empty space, drag to resize

I love writing in the morning. Ideally I’m up before the kids, with a coffee and a few minutes of meditation before sitting down to write. Of course, that plan doesn’t always work...sometimes the morning writing session turns into a shared workspace with cartoons and stuffed animals.
Empty space, drag to resize
Over the past month I’ve started venturing into male pelvic health. After 13 years focused mostly on pain, it has been refreshing, and humbling, to explore a new area of practice.
For pelvic health clinicians reading this, what follows will not be new. But for many clinicians in musculoskeletal care, it might be.
One statistic that caught my attention: about 1 in 9 men will develop prostate cancer in their lifetime in Canada. Many of these men will undergo radical prostatectomy, and when the cancer is localized the 5-year survival rate is close to 100%.
In other words, the surgery is often very successful. But survival is not the whole story.
For many men, the journey really begins once men hear the "C-word" and after the surgery, regaining continence, erectile function, and confidence, is another challenge to venture into.
This week I went down the rabbit hole on the rehabilitation side of radical prostatectomy, particularly the work of Jo Milios and colleagues looking at pelvic floor muscle training (PFMT) before and after surgery.
GI Disorders in Pelvic Health with Dr. Susan Clinton
Tall Tree Health Cordova Bay: September 18 and 19, 2026
Learn how to assess and treat common GI issues like constipation, bloating, and bowel dysfunction using an integrated gut–brain–pelvic health approach.
Hybrid Course Design:
- 6 hours pre-course videos + articles
- 2 day In Person Workshop: Lecture, Lab, Discussion
- 2 Virtual Follow-Up Calls
- $840
- 10% discount until March 31, 2026 = Use GI10 at Checkout

The part that surprised me most was not the role of pelvic floor rehab.
It was how long erectile recovery can take.
In the
Milios 2020 trial, men began pelvic floor training about
five weeks before surgery and resumed the program once the catheter was removed.
The higher-intensity group performed:
• 6 sets per day
• 10 quick contractions (1 second)
• 10 endurance contractions (10 seconds)
That’s 120 pelvic floor contractions per day, performed in standing.
This is not vague advice to “do some kegels.” This is structured neuromuscular training that is going to take some serious time and effort.
What also stood out was the recovery timeline.
Even with nerve-sparing surgery, research suggests that only 16–22% of men return to their baseline erectile capacity by two years, and many men continue recovering for three to four years after surgery.
That timeline surprised me.
In musculoskeletal rehab, we often think in terms of weeks to months, maybe a year.
Here we are talking about years.
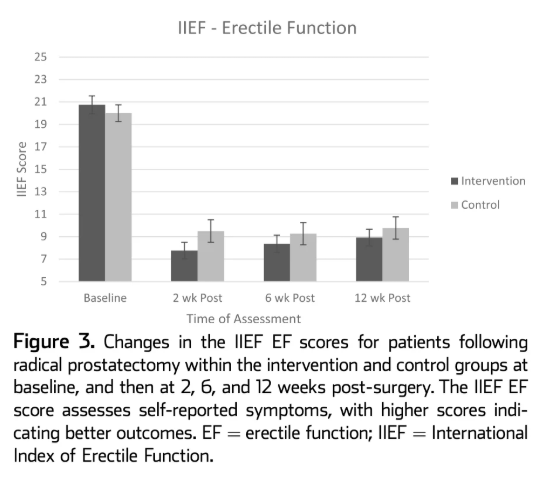
From
Milios et al. 2020. Erectile function drops sharply after surgery in both groups and shows only modest recovery by 12 weeks, highlighting the slow and incomplete early return of erectile function after prostatectomy.

Pelvic floor muscle training after radical prostatectomy is about 3 things at the least:
- Regaining continence
- Regaining erectile function
- Rebuilding confidence
The pelvic floor muscles, particularly the bulbocavernosus and ischiocavernosus contribute to penile rigidity by increasing intracavernosal pressure and supporting venous occlusion.
Several studies suggest PFMT may help improve erection quality, especially when started before surgery and resumed soon after catheter removal.
But erectile recovery after prostatectomy is a long road. Even with nerve-sparing surgery, many men take 12–24 months to regain meaningful erectile function, and some never return fully to baseline. For all those folks with prostates out there, let that sink in for a moment.
Part of the challenge is that erectile rehabilitation depends on re-engaging with sexual activity.
This is where continence recovery becomes more important.
Faster continence recovery may reduce barriers to sexual activity and help men engage in penile rehabilitation sooner, although the causal link between continence recovery and erectile recovery has not been definitively established.
In practice, here's what's going on...
Many men experience urinary leakage after surgery, including climacturia (urine leakage during orgasm). Attempting sexual activity while worrying about urine leakage, wearing pads, or losing bladder control can be deeply uncomfortable and embarrassing. For many couples, the result is simple: They avoid sexual activity altogether.
This matters because penile rehabilitation aims to keep erectile tissue healthy and oxygenated while nerves recover from surgical trauma.
Common strategies include:
- PDE5 inhibitors (sildenafil, tadalafil)
- Vacuum erection devices
- Graded return to sexual stimulation and intimacy
- Intracavernosal injections
Without erections or stimulation, penile tissue can undergo reduced oxygenation, smooth muscle loss, and fibrosis, which may contribute to long-term erectile dysfunction.
Empty space, drag to resize
A patient story...
A 62-year-old man returns 6 weeks after prostatectomy. His cancer surgery went well, but he is using 3–4 pads per day and leaks when he coughs, bends, or stands quickly. Sadly, he can only drink 1 coffee per day or leaking gets worse. On Thursday, he typically loves going to the pub for a beer with colleagues but this too is tough to handle. Lots of change.
When asked about sexual activity he laughs awkwardly and says,
"That’s the last thing on my mind right now."
Later his partner admits they are both worried about urine leakage during intimacy.
Until continence improves and confidence returns, sexual rehabilitation simply may not start.
Improving continence earlier and keeping penile rehab in view can help remove one of the biggest psychological and practical barriers to restarting intimacy and improving a patient's quality of life.

If you work with men undergoing radical prostatectomy, one of the biggest shifts might be to think in terms of a
rehabilitation timeline rather than isolated exercises.
A simplified model looks like this.
Pre-operative phase (4–6 weeks before surgery)
Teach pelvic floor anatomy, coordination, relaxation, and both quick and endurance contractions. Get those going sooner rather than later. Introduce how to regain continence and sexual function after surgery.
Early post-operative phase (after catheter removal)
Resume pelvic floor training with structured sets of quick and endurance contractions. Start talking about
Months 3–12
Continue to combine pelvic floor rehab with penile rehabilitation strategies and gradual return to sexual activity.
For clinicians who treat musculoskeletal conditions, this can feel surprisingly familiar.
It’s essentially prehab + rehab + graded exposure, just applied to a different part of the body. It's not that simple, but you get the gist.
Dry Needling Refresher Courses
Nanaimo, BC: April 12, 2026
Whitehorse, Yukon:
October 24 & 25, 2026...two full days of live needling reps.

Prota et al., 2012
Randomized trial showing pelvic floor muscle training after catheter removal improved erectile recovery at 12 months compared with usual care.
Lin et al., 2012
RCT demonstrating lower rates of erectile dysfunction in patients completing pelvic floor training after radical prostatectomy.
Geraerts et al., 2015
Showed pelvic floor muscle training can improve erectile function and climacturia even when started more than a year after surgery.
Taken together, these studies highlight something important:
Pelvic floor rehabilitation is not just about pads and continence.
It is increasingly being viewed as part of sexual rehabilitation after prostate cancer treatment.
For clinicians used to treating musculoskeletal injuries, the concepts are surprisingly familiar: prehabilitation, neuromuscular retraining, graded exposure, and long-term recovery timelines.

One idea kept coming back to me while reading this literature.
Radical prostatectomy is often framed as a cancer surgery. But functionally, it’s also a nerve injury.
During surgery, even with nerve-sparing techniques, the cavernous nerves that control erections are stretched, compressed, and temporarily stunned. Again, this phenomenon called neuropraxia, can take months to years to recover.
While those nerves are recovering, the penis may spend long periods without normal erections, which means less oxygen delivery to the erectile tissue. Over time this can lead to smooth muscle loss, fibrosis, and reduced erectile capacity.
This is why penile rehabilitation exists. The goal isn’t just to restore erections. The goal is to keep the tissue healthy while the nerves heal.
And that changes how you think about rehabilitation. Instead of asking “When will erections come back?” the better question becomes:
“What can we do now to preserve function while recovery unfolds?”
That small shift, from waiting for recovery to actively promoting function, is what makes pelvic health rehabilitation such an important part of prostate cancer care.
Empty space, drag to resize
I have a lot more to learn in this area, and I’m sure I’ll make a few mistakes along the way. There’s a bit of imposter syndrome that comes with stepping into a new field after 13 years in pain care, but I’m excited for the journey ahead.
What has struck me already is how meaningful this work can be. For many men, the cancer treatment may be successful, but the return to continence, intimacy, and confidence takes time.
Being part of that recovery journey is important work, and I’m grateful to be learning from the pelvic health clinicians and scholars who have been doing it well for years.


{kind=link}
