Empty space, drag to resize
Hey folks,
This week, we’re bringing you the largest-ever study on menopause in BC — and why it matters in rehab.
The HER-BC Report (2024), led by Dr. Lori Brotto and the Women’s Health Research Institute, is a landmark mixed-methods study of 2,133 midlife individuals assigned female at birth across British Columbia.
It sheds critical light on how menopause symptoms intersect with physical, psychological, and social health — and how stigma, lack of preparation, and fragmented care continue to leave people unsupported.
This isn’t just a women’s health issue.
It’s a workforce issue, a rehab issue, and a systems issue.
The study combines:
- Deep survey data
- Validated scales (PHQ-9, GAD-7, MRS, MENQOL)
- In-depth interviews
Together, these uncover how menopause impacts everything from quality of life to mental health, caregiving burden, and functional participation — especially at work.

We’ve long been taught to associate menopause with vasomotor symptoms — hot flashes, night sweats, and hormonal shifts.
But the real picture is much more complex — and often invisible to providers.
Menopause is:
- Exhaustion that doesn’t lift with rest
- Joint and muscle pain that defies biomechanical explanation
- Cognitive fog that chips away at confidence
- Mood instability in people with no prior history of mental illness
- A loss of bodily trust that feels disorienting, even frightening
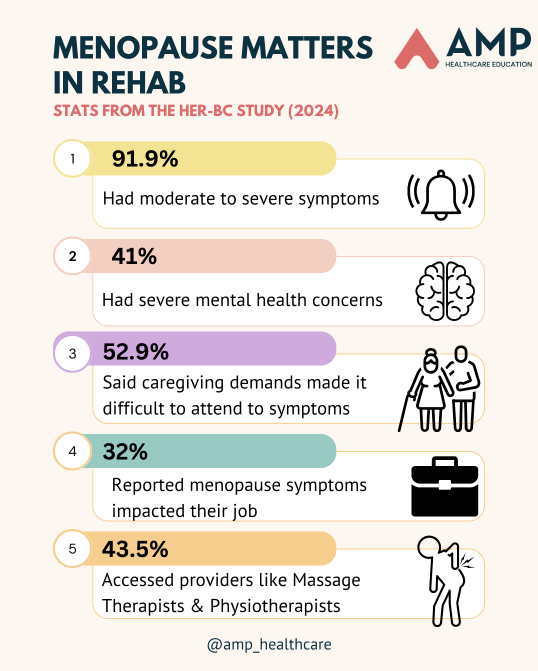
📊 Key insights from HER-BC:
- 92% of participants reported at least one moderate to severe symptom
- Nearly half lived with a chronic health condition
- Symptom severity was moderately correlated with depression, anxiety, loneliness, and poor quality of life
- 1 in 3 said symptoms affected their ability to work
Many didn’t realize they were in menopause until symptoms were debilitating. Others said they were dismissed by providers or told it was “just stress” or “normal aging.”
Some quit jobs. Others passed on promotions or left the workforce entirely.
This was really stood out for me...
The sheer volume of people who said:
“No one told me this was coming. I thought I was going crazy.”
This report is a wake-up call for rehab professionals.
Menopause isn’t a side issue. It shows up in our caseloads every single day — we just haven’t been naming it. It’s seeing us, we’re not seeing it. Until now.

Rehab professionals — especially physiotherapists, occupational therapists, and RMTs — are in a unique position to recognize, validate, and support people navigating menopause.
Why?
Because we often treat the symptom-level fallout of unrecognized hormonal transitions:
- Persistent low back, lateral hip pain or pelvic pain
- Sudden joint instability or hypermobility
- Sleep disturbances and chronic fatigue
- Urinary urgency, leakage, or prolapse symptoms
- Feelings of being “off,” unmotivated, or emotionally dysregulated
- Trouble engaging in work, exercise, or caregiving roles
But without recognizing the underlying context — hormonal transition — we risk:
- Treating in isolation, focusing on tissues instead of the whole person
- Missing key contributors to distress or functional loss
- Reinforcing internalized messages that people should “just push through” or “get back to normal”
Menopause doesn’t always present with a clear “chief complaint.”
But it often hides in the complexity — in the slow shifts, the invisible barriers, the subtle unraveling of function.
📌 Also important:
Many people are turning to rehab providers first — because they can’t access or don’t feel supported by their primary care team.
We are increasingly seen as entry points to care — and that makes menopause our business.

If you’re not screening for menopause-related changes, you might be missing an opportunity to frame your care more holistically.
Have you ever had a client say:
“I don’t feel like myself lately.”
“My pain’s not that bad, but I’m just so tired.”
“It’s like my body isn’t mine anymore.”
These aren’t just physical complaints. They often point to identity-level disruption.
And they deserve to be explored with curiosity, not minimized or psychologized away.
Ask yourself:
- Do I ask about menstrual changes in my intake?
- Have I been trained to consider hormonal transitions in pain, fatigue, and recovery patterns?
- Do I normalize conversations around midlife, identity, and change?
If not — you’re not alone. But this is your moment to get more informed.

🔎 Rehab Implications
Menopause is not just a gynecological issue. It shows up in:
- The shoulder that suddenly won’t settle.
- The runner with new hip pain and sleep disruption.
- The parent struggling to regulate mood while caregiving.
- The high-functioning professional whose executive skills are slipping.
Practical shifts to make now:
- Expand your symptom radar: Fatigue, cognition, dizziness, and emotional volatility can all be menopause-related.
- Be a connector: Help clients make sense of their experience — even if you’re not the hormone expert.
- Ask about work: Menopause-related disruptions at work are real. Can you support with pacing, accommodations, ergonomics, or mindfulness-based strategies?
🔎 Big Picture
This is bigger than individual care. It’s about creating systems and services that recognize and validate the midlife transition.
Menopause care needs to be:
- Multidisciplinary (pelvic health, MSK, mental health, lifestyle, nutrition)
- Culturally informed (not everyone experiences menopause the same way)
- Trauma-informed (especially for those with body-based trauma histories)
- Proactive rather than reactive
Rehab is well-positioned to lead — but we need to stop waiting for referrals and start integrating menopause into our everyday lens.

“It’s like hitting a brick wall and not coming out the same person at the other side. And nobody prepares you for it quite the way it happens.”
— age 52, HER-BC participant
This line stopped me in my tracks.
Because rehab is so often about what happens after the wall:
- After the injury.
- After the identity shift.
- After the loss of control.
What if we became the clinicians who meet people in the rubble — and help them rebuild?
Not by offering fixes.
But by offering language. Options. Grounding. Possibility.
📖 Want to dig deeper?
Read the
HER-BC Report - it’s thorough, illuminating, and loaded with insight.
Whether you’re new to menopause-informed care or deep into pelvic health, this will expand your lens.
💬 Favorite interview quote:
“I started to think I was just weak. I didn’t know it could be menopause.”
Let’s make sure people don’t walk through this season alone, uninformed, and unsupported.
