Empty space, drag to resize
A patient came in a week ago with medial knee pain. It first showed up after ramping the running mileage up, recovered on its own, then came back a month later. Frustrated, he decided to experiment with peptide BPC-157: four injections a week for four weeks into the lateral quadricep. Over that month the knee slowly improved, and he was sold. Three months later the pain is back, which is why he is now sitting in front of me. It is a small story, but it lends insight into a few things worth thinking through about peptides entering the rehab space.

First, how people think peptides work, because the theory is genuinely appealing. The peptide most are talking about is BPC-157, a 15 amino acid chain originally isolated from gastric juice.
The proposed mechanism:
- It promotes the growth of new blood vessels into poorly perfused tissue like tendon
- Dials down inflammation, and nudges fibroblasts to migrate and lay down collagen.
In other words, the pitch is that you inject a healing signal directly at the site, and the body's repair machinery gets switched on and accelerated. For someone with a stubborn knee that keeps flaring, that is a very attractive idea.
There are now roughly 200 studies on peptides in
PubMed, and on paper the story appears to hold up: faster healing of tendon, ligament and muscle in animals, driven by the aforementioned mechanisms. The
Achilles transection work in rats is the headline finding, alongside similar results in
ligament models.
Two things are worth thinking on here.
- First, almost all of this is animal research, and the great majority of it comes from a single lab in Croatia, with a second supporting group in Taiwan. That is not automatically disqualifying, but when one team produces most of the positive findings on a compound they also hold patents on, reviewers reasonably start asking about confirmation bias.
- Second, the human data is thin to the point of being almost absent. Fewer than 30 people across a handful of published pilot studies, none with a proper comparison group, and one registered trial whose data was withdrawn before outside review.
Animal models are genuinely useful. They let you control the injury, the timing and the dose, and they reveal mechanism in a way you can never do in a clinic. But the translation graveyard is enormous. As one physician put it, we have cured cancer in mice plenty of times and have not done it in people yet. Rodents heal differently, are dosed differently, and do not carry the years of load, fear and deconditioning that walk into our rooms.
What looks promising in a rat is still only a hypothesis about humans. It is not a result.

Biological plausibility is seductive because it sounds like proof, but it is only a starting point. The clearest cautionary tale we already have is PRP.
Quick correction on the mechanism:
- PRP is not injected cells, it is a patient's own concentrated platelets and growth factors, spun from their blood and put back in. But the logic is the same as the peptide pitch.
- Take something that signals healing, inject a single bolus at one arbitrary moment, and hope it slots neatly into a healing cascade that unfolds over weeks in phases.
When that idea was tested properly, PRP did
no better than a saline injection for Achilles tendinopathy. *The plausible story did not survive a placebo*. There is no strong reason to assume peptides will behave differently until someone runs the trial. Layer on the fact that many musculoskeletal injuries improve on their own (natural history) and the expectancy bias, it is hard to to untangle what the peptide may or may not be doing.
My runner is good illustration of this. His knee had already shown it could settle and flare on its own before he ever touched a peptide. It improved during the four weeks he injected, then returned three months later. The simplest read is not that the peptide worked and wore off. Perhaps he may of caught another normal dip in an up and down condition, credited the injections, and the underlying driver, a sharp spike in load his tissue was not ready for, remained unaddressed.
Also, since this condition is recurrent, we know a good next step is to follow the
evidence. There is good data that suggests specific education around load management, reassurance, and a few hip and knee exercise can work wonders for many. Time will tell if this approach creates a more durable recovery over the peptide.
"*PRP is a very messy body of research. Variability in preparation methods, platelet concentration, dosing, timing, injection protocols, and patient selection makes studies difficult to compare. Many trials are underpowered, with sample sizes of fewer than 20–30 participants, and are often limited by methodological weaknesses, risk of bias, and inadequate comparison groups. As a result, it remains challenging to determine whether PRP provides meaningful clinical benefit for many conditions. Despite this uncertainty, PRP is widely marketed for a broad range of indications, including erectile dysfunction, vaginal rejuvenation, hair loss, tendinopathies, Alzheimer's disease, autism, chronic Lyme disease, and many others.
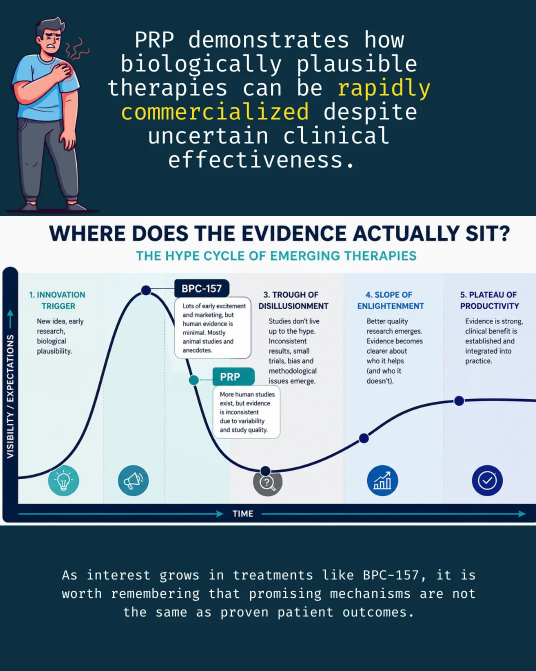
While PRP has at least been studied extensively in humans, it serves as a cautionary example of how biologically plausible therapies can be rapidly commercialized long before clinical effectiveness is clearly established—a lesson that may be relevant to emerging treatments such as BPC-157.*"

If your patient is using or set on trying, I think there are three things worth raising:
- Be honest about the evidence. The interesting findings are almost all in rats. That data is being extrapolated to humans, but the human trials largely haven't been done, so nobody actually knows how this plays out in people. Say it plainly: promising in animals, unproven in humans.
- Know what's in the vial. This is an unregulated market, so the near-term risk usually isn't the peptide, it's contamination and inaccurate dosing. If they're going to use, push them toward third-party purity and sterility testing of the actual product they have.
- Route matters. If they're injecting, caution strongly against intraarticular (into the joint) injections because of the obvious joint infection risk. Septic arthritis is not a problem you want to chase. Intramuscular or subcutaneous is the safer floor. Worth pointing out too: the studies they're citing usually inject in the abdomen or systemically, nowhere near the joint, so "putting it where it hurts" isn't even what the research did.
None of this is endorsement. It's harm reduction plus modelling good reasoning, and it's a fair moment to loop in their physician or pharmacist on the testing and route questions. You stay credible, they stay safer, and the door stays open for the next conversation.

The researchers surgically cut through the Achilles tendon of rats, leaving a visible gap, then dosed them once daily with BPC-157 in saline or saline alone. Importantly the peptide went in via the abdominal cavity, not locally into the tendon, starting 30 minutes after surgery.
Over 14 days the treated tendons healed better on every measure: stronger and stiffer biomechanically, better walking scores, more organised collagen with less inflammation, and a smaller defect. The saline controls healed poorly. It is a positive result.
Now notice how far it sits from the runner I had last week.
This is a freshly severed tendon, an acute surgical laceration, not gradual load-driven knee pain. It is systemic dosing in a rat begun minutes after a clean cut, not an injection near a joint months into a flare, and the whole story plays out in two weeks.
That gap between the model and the patient is the entire point.
For the wider context of how this one line of research became a wellness phenomenon, the
Undark investigation co-published by STAT is a good companion read. It traces the literature back to a single Zagreb lab holding patents on the compound, lays out the 2023 FDA move to stop pharmacies compounding it over impurity and immune concerns, and quotes a USADA scientist on what an unregulated vial might contain: "a peptide, a steroid, or something just like water."


"We've cured cancer in mice plenty of times. We haven't done it in people yet."
It's a throwaway line, but it captures something fundamental about how humans think. We are naturally drawn to compelling stories, especially when they offer a shortcut through uncertainty. Animal studies tell us something might work and provide clues about how it works. They do not tell us whether it will work in humans, in whom, at what dose, or at what cost. This is not cynicism...it is respect for how difficult biology is and how hard healing is to engineer.
The attraction of peptides makes sense. When we are injured, in pain, or frustrated, we want to fix the tissue and move on. We prefer the promise of a targeted solution over the slower reality of adaptation. Yet much of human recovery does not come from being fixed. A vial purchased online, of uncertain purity, injected near a joint at the kitchen table carries real risk for a benefit we cannot yet confidently measure.
At the same time, healthcare should remain open to innovation. Our current tools do not help everyone, and many of today's accepted treatments began as novel ideas that challenged conventional thinking. New therapies may eventually prove valuable and expand what we can offer patients. The challenge is balancing curiosity with discipline. History is full of promising interventions that generated excitement long before the evidence arrived, and some never delivered on their promise. We should be careful not to let enthusiasm for the next breakthrough distract us from first-line treatments that already have strong evidence and help many people every day.
Curiosity about the science and caution about the practice are not opposing positions. They are both expressions of good clinical reasoning. The challenge is resisting the very human urge to mistake a promising story for a proven outcome.
Stay nerdy,
