Empty space, drag to resize
I have been spending a lot of time lately in unfamiliar territory. Men's health, and specifically male pelvic pain, is a space I am two months into. I will share a story in this newsletter on how I probably got here.
But I recently returned from a course with
IPC Health focused on Male Pelvic Pain, and I left with energy with a mind that was full. What's landed is the diversity of stuff that men are carrying, often for years, even decades, without ever having a conversation about it with a clinician.

Here is a sample of what has been landing in my clinic lately:
- Men preparing for radical prostatectomy who need pre-op pelvic floor education and training before prostate cancer surgery.
- Men post Green Light laser ablation dealing with urinary incontinence and difficulty achieving and maintaining erections.
- Men noticing seminal fluid leaking after urination.
- Perineal pain with sitting and walking.
- Men struggling with premature ejaculation who have never spoken to a clinician about it.
These are not rare presentations. They are common, appear to be undertreated and quite medicalized, and not often referred to physio. Most of these men have had lots of medical testing and medications, but are unsure of next steps once those options have been explored.
Around 70% of men presenting with pelvic floor complaints - pain in the penis, testicle, or perineum during walking, sitting, sex, masturbation, urination, or defecation, have a lumbar spine contributor to their experience.
It's surprising because these presentations feel so somatic, so localized. The idea that the lumbar spine is driving or maintaining that pain for the majority of them challenges the instinct to go straight to tissue and once again, just pause when we start going down the pathoanatomy rabbit hole.
If you treat musculoskeletal complaints, regional interdependence in play here too. Just like the neck influences the shoulder and upper limb of the hip influences stuff at the knee, we have lower back issues influencing the pelvis.
The pelvic floor, in part, seems to be a new context for an old truth.
The piece that really caught my attention from what exists in the literature, and what I heard on course, is that many of these men can make meaningful change or in some cases, completely solve their symptoms without any direct pelvic floor work at all. The mechanism isn't manual therapy to the levators or a progressive loading program for the pelvic girdle. It's something more familiar: finding a directional preference.
A movement, a position, a loading strategy that reproducibly shifts their symptoms. Something that puts them in the driver's seat. This is a concept most of us know from lumbar care, but in male pelvic pain it can carry some weight because these men have often been told nothing can be done, or that they need to Kegel or just down train the pelvic floor.
Finding a direction that creates change is evidence. It says: this is responsive. You can influence it. That changes everything about how a patient relates to their own body. It's also a great place where therapists can intervene (TLJ, lumbar spine, LSJ, and glutes).
A
2018 case series by Wu and Rosedale in Physiotherapy Theory and Practice illustrates this well. Three men presented with lower urinary tract symptoms as their primary complaint: frequency, urgency, nocturia, dysuria, weak stream. Urological pathology had been ruled out for all of them.
All three were classified as lumbar derangements through MDT assessment. Two had a directional preference for extension, one for flexion. Average improvement on the NIH Chronic Prostatitis Symptom Index was 65%, over an average of six sessions.
One of the men had two to three years of testicular and prostate region pain alongside his urinary symptoms. His first week of flexion-based exercises produced almost no low back pain and only one episode of testicular pain. He was discharged with near-normal urinary frequency and describing himself as pain free most of the day.
It is a case series of three. The evidence base in male pelvic pain is thin enough that this qualifies as a needle in a haystack. But it is a useful proof of concept: the lumbar spine is worth assessing in these men, and the tools to do that assessment are already in most physio clinics.
What I did not expect, two months in, is how much of what I already know applies here. A good orthopaedic background turns out to be real preparation for men's pelvic health. The assessment logic is familiar. Load management, graded exposure, movement analysis, understanding how the nervous system contributes to a pain experience, how to have a conversation about sensitive symptoms without making it strange, all of it transfers.
The anatomy is different and some of the presentations are unlike anything in a typical MSK caseload. Definitely more medical team involvement. But the clinical reasoning underneath them is not. I am not starting from scratch. I am applying what I know in a space that badly needs more clinicians willing to show up. That said, I still have tons to learn.

Directional preference exercises are not a magic bullet. Male pelvic pain is phenotypically diverse, and the lumbar spine is one contributor among many.
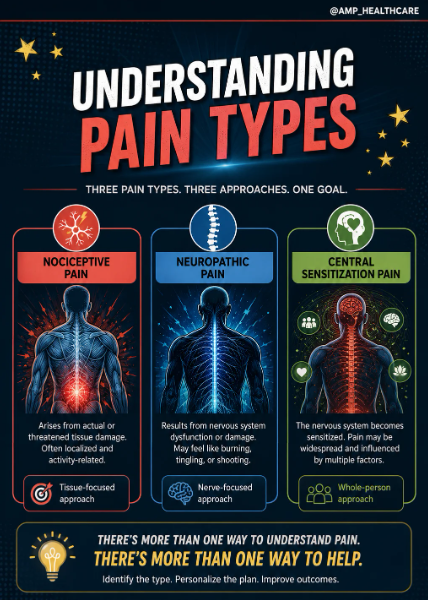
Some presentations are:
- Primarily nociceptive and mechanically driven.
- Others are nociplastic: central sensitization, widespread sensitivity, IBS, migraines, fibromyalgia, and pain that doesn't follow rules.
- Others have a clear neuropathic component, or have
- A significant psychosocial load that no directional exercise will touch.
Phenotyping matters here. The MSK orthopedic reasoning transfers well, but it has to be applied with the same critical thinking you'd use anywhere else: assess, attempt to classify, trial, and watch what happens.
If the lumbar screen moves the needle, keep going. If it doesn't, that's information too - and a reason to refer sooner rather than later to someone with specific pelvic health training. The point isn't that you can treat everyone. It's that the assessment is worth doing.

About 10 years ago, I was treating a young guy for low back pain. Pretty standard case, we were six weeks in, near the end of care, and he mentioned almost in passing:
"My back pain is gone, and I don't have painful erections anymore."
He'd never mentioned the erection pain. I hadn't asked. And somewhere in the course of treating his back, that had resolved too.
My interest was piqued. I started digging into the research, looked at a few courses… and then, for whatever reason, set it aside. But that moment stuck with me, and kept me interested in the pelvic health domain since.
Here's the takeaway:
If you see patients with low back or hip pain, ask whether they've noticed any pelvic, groin, or perineal pain, or any bladder, bowel, or sexual health changes, since the onset of their issue. If they have, there's a chance that adding a simple directional assessment might help before you assume the problem lives in the pelvic floor.
Run them through a few repeated movements or positional changes and ask how it affects their symptoms as you move through a course of care. You don't need pelvic floor training to start here. You're looking for something that moves the needle, even slightly. If you find it, you've already begun treatment. If it plateaus, refer to a pelvic health provider.
The screening question costs you nothing. The answer might change everything.

1. Wu & Rosedale (2018),
"The use of Mechanical Diagnosis and Therapy (MDT) in patients with lower urinary tract symptoms: case series," Physiotherapy Theory and Practice. Three men, urological pathology ruled out for all, all classified as lumbar derangements through MDT assessment. Average improvement of 65% on the NIH Chronic Prostatitis Symptom Index over six sessions. It's a case series of three, and the authors are the first to say that. But it's worth reading if you do lumbar care and want to see how this transfer of reasoning looks in practice. The mechanism is still poorly understood. The clinical signal is worth taking seriously.
2. Review the nerves of the lower back and pelvis.
I created this visual with the help of ChatGPT to make the lumbosacral plexus a little easier to understand and remember clinically. From the pudendal nerve to the sciatic nerve, these structures can influence pain, movement, continence, sexual function, and pelvic floor behaviour more than many clinicians realize.
Inside you’ll review common nerves and their spinal segments, including:
- Lumbosacral trunk (L4–L5)
- Superior gluteal nerve (L4–S1)
- Inferior gluteal nerve (L5–S2)
- Pudendal nerve (S2–S4)
- Posterior femoral cutaneous nerve (S1–S3)
- Sciatic nerve (L4–S3)
- Common fibular division (L4–S2)
- Tibial division (L4–S3)
I’ve taken their pain course, completed the free anatomy course, and purchased the erectile dysfunction course as well. These folks are true nerds with passion: thoughtful, evidence-informed, and genuinely excellent educators.
Worth following if you want to sharpen your understanding of pelvic pain, pelvic floor dysfunction, sexual health, and the overlap between the lumbar spine and pelvis.

Pelvic health care is so much more than simply “uptraining” or “downtraining.”
Pelvic presentations can involve understanding the story, good planning, the nervous system, the lumbar spine, the pelvic floor, movement behaviours, sensitivity, strength, stress, breathing, beliefs, load tolerance, continence, sexual function, partners, pain science and other things.
- Some patients need calming.
- Some need capacity.
- Some need confidence.
- Some need a better map of what is happening in their body.
Sometimes even a small directional preference or symptom change with movement becomes meaningful. When symptoms shift, even slightly, patients often realize for the first time that their body is responsive, that they can influence it. For people who have spent years feeling stuck, that discovery alone can change the trajectory of care.
Phenotype matters. Context matters. The person matters.
The goal is not to force everyone into the same recipe. The goal is to understand the presentation in front of you well enough to help guide the next right step.
There is no one-size-fits-all approach in healthcare. Good care lives in the nuance. Let's stay there.

{kind=link}
{kind=link}